You have heard that laughter is the best medicine, but have you dwelt on how laughter heals?
Let's start with the admission that pain and suffering exists, which his why we need healing at all. Medical doctors have determined that there is truth in the expression that laughter functions like medicine. But I'm not talking about acute medical problems. I'm interested in relief from existential dread. We live in a world where the Ignorant are in charge and fully committed to setting the conditions for maximal, pervasive distress. Given the severity of the wound, we're going to need a lot of laughter. As I argue in my new book, we need a certain kind of laughter, one that fully embraces the pain as it simultaneously points the way to a new mode of being.
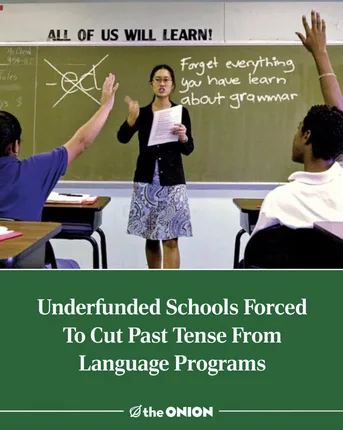
Consider the headline from The Onion above. Again, let's start with suffering. The joke hurts because it presses on a few sore points. First, schools aren't really helping young people learn how to learn. Kids are great at doing school, but, as Mark Twain pointed out long ago, that skill is actually getting in the way of education. So, on one level, the headline hurts because it reminds us that the institution of education in the U.S. has largely failed to cultivate new generations of critical thinkers. Second, of all the subjects of study to lose their grip within the halls of primary and secondary education, history is perhaps the one we ought to grieve the most. True, the joke appears to be about literacy and grammar. But by cutting the "past tense," that means that not only will students need to learn how to read in a new way but they will also lose access to the past. Level two of the joke appears here: we've already lost access to that. Texas textbook revisionism coupled with too strong of a reliance on logical positivist approaches to the past has created a shallow presentism. If history seems to repeat itself, that's because we, as a nation, can't seem to recall the history of mistakes we keep making and the poor decisions we keep making on purpose. Third, and finally, the joke hurts because funding cuts are now chipping away at our vocabulary. If we cut the past tense out of our language, that'll let us function on only 2/3 of our budget, right?
Wrong. And yet we laugh. What kind of laugh does The Onion produce here? I call the kind of humor at work here a humor of congruence. Dialectically related to the dominant incongruity theory humor, which states that comedy often arises from the incommensurability of two or more side-by-side people, ideas, or situations, my congruent theory of humor suggests we laugh when something reveals precisely how something is. The formula shifts from "this does not equal that" to "this is this." In the headline, even though the scenario is exaggerated, the exaggeration reveals precisely what is the case; namely, the headline reveals how bad off we are in the present due to the failings of the educational institution. The laugh produced astride the recognition of what is the case is a laugh of recognition, and recognition is the first step toward healing. We can't get get better if we don't know we're sick.
Let's start with the admission that pain and suffering exists, which his why we need healing at all. Medical doctors have determined that there is truth in the expression that laughter functions like medicine. But I'm not talking about acute medical problems. I'm interested in relief from existential dread. We live in a world where the Ignorant are in charge and fully committed to setting the conditions for maximal, pervasive distress. Given the severity of the wound, we're going to need a lot of laughter. As I argue in my new book, we need a certain kind of laughter, one that fully embraces the pain as it simultaneously points the way to a new mode of being.
Consider the headline from The Onion above. Again, let's start with suffering. The joke hurts because it presses on a few sore points. First, schools aren't really helping young people learn how to learn. Kids are great at doing school, but, as Mark Twain pointed out long ago, that skill is actually getting in the way of education. So, on one level, the headline hurts because it reminds us that the institution of education in the U.S. has largely failed to cultivate new generations of critical thinkers. Second, of all the subjects of study to lose their grip within the halls of primary and secondary education, history is perhaps the one we ought to grieve the most. True, the joke appears to be about literacy and grammar. But by cutting the "past tense," that means that not only will students need to learn how to read in a new way but they will also lose access to the past. Level two of the joke appears here: we've already lost access to that. Texas textbook revisionism coupled with too strong of a reliance on logical positivist approaches to the past has created a shallow presentism. If history seems to repeat itself, that's because we, as a nation, can't seem to recall the history of mistakes we keep making and the poor decisions we keep making on purpose. Third, and finally, the joke hurts because funding cuts are now chipping away at our vocabulary. If we cut the past tense out of our language, that'll let us function on only 2/3 of our budget, right?
Wrong. And yet we laugh. What kind of laugh does The Onion produce here? I call the kind of humor at work here a humor of congruence. Dialectically related to the dominant incongruity theory humor, which states that comedy often arises from the incommensurability of two or more side-by-side people, ideas, or situations, my congruent theory of humor suggests we laugh when something reveals precisely how something is. The formula shifts from "this does not equal that" to "this is this." In the headline, even though the scenario is exaggerated, the exaggeration reveals precisely what is the case; namely, the headline reveals how bad off we are in the present due to the failings of the educational institution. The laugh produced astride the recognition of what is the case is a laugh of recognition, and recognition is the first step toward healing. We can't get get better if we don't know we're sick.

As a mental health counselor, I often bring this theory of humor into the group therapy environment. I distribute humorous images and wait for the laughter to erupt. Once people laugh, I ask the question: what's so funny? Take this Alice In Wonderland image, for example. The theory of incongruity suggests that the humor arises from the divergent meanings of "mad." The Cheshire Cat means "we're all crazy here," but Alice thinks she's done something wrong: Are you "mad" (Angry) at me? But this incongruity (mad ≠ mad) is not the only reason, or even the main reason that healing laughter arises after encountering this meme.
Whether we're in a therapeutic setting or not, insecurities abound. Insecurities come from beliefs about ourselves that we safeguard and try to keep from view. Despite our best efforts, however, the beliefs do in fact show themselves, often through our speech and our behavior. When Alice interprets the cat's "mad" to mean that she's already done something wrong, she is showing us one of her insecure beliefs. She must have done something wrong because that's her thing. She's the one who has always already done something wrong. And the cat et al. know it. In my group therapy sessions, people laugh as they identify themselves with the same core belief. If people don't have that core belief, they tend not to "get" the joke right away. People who suffer from this kind of insecurity access the healing laughter first, maybe because they're the ones who need it. Presumably, the person who made this meme is one of these insecure people. It was made for the purpose of naming this common problem. What is the case? Many people enter spaces with the presumption that they are in the wrong and that everyone either knows it already or will soon find out.
Invisible and privately held beliefs become visible, and the healing begins. I feel like Alice. Oh, you, too? Oh wait, whoever made this meme really gets it. There's a whole community of us! Uh oh, that's not good. This feeling is a thing. A common thing? Is that what this group is about? Of course it is. I'm laughing in multiple ways now. I "get" the joke + the joke's on me + the joke's not funny + I'd rather not be the person who gets the joke. Do I drink alcohol because I feel this way? No. That's can't be it. Is it?
Step two of the healing process of this particular kind of laughter reveals itself at this point. Step 1: laughter makes what it is the case visible. Step 2: once visible, laughter unites people who typically suffer in silence and alone.
Whether we're in a therapeutic setting or not, insecurities abound. Insecurities come from beliefs about ourselves that we safeguard and try to keep from view. Despite our best efforts, however, the beliefs do in fact show themselves, often through our speech and our behavior. When Alice interprets the cat's "mad" to mean that she's already done something wrong, she is showing us one of her insecure beliefs. She must have done something wrong because that's her thing. She's the one who has always already done something wrong. And the cat et al. know it. In my group therapy sessions, people laugh as they identify themselves with the same core belief. If people don't have that core belief, they tend not to "get" the joke right away. People who suffer from this kind of insecurity access the healing laughter first, maybe because they're the ones who need it. Presumably, the person who made this meme is one of these insecure people. It was made for the purpose of naming this common problem. What is the case? Many people enter spaces with the presumption that they are in the wrong and that everyone either knows it already or will soon find out.
Invisible and privately held beliefs become visible, and the healing begins. I feel like Alice. Oh, you, too? Oh wait, whoever made this meme really gets it. There's a whole community of us! Uh oh, that's not good. This feeling is a thing. A common thing? Is that what this group is about? Of course it is. I'm laughing in multiple ways now. I "get" the joke + the joke's on me + the joke's not funny + I'd rather not be the person who gets the joke. Do I drink alcohol because I feel this way? No. That's can't be it. Is it?
Step two of the healing process of this particular kind of laughter reveals itself at this point. Step 1: laughter makes what it is the case visible. Step 2: once visible, laughter unites people who typically suffer in silence and alone.
Step 3: Healing doesn't just happen. You make it happen.
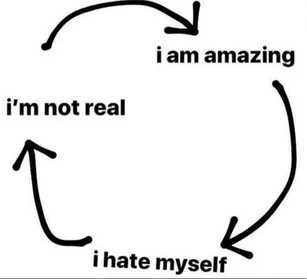
Once something typically hidden becomes visible and we verify that, yes, this is the case, and once we unite with others who suffer in similar ways with us, then we can turn to the work of producing healing. One of the many drawbacks of Western medicine's reliance on pharmacology is that the pervasiveness of pills and prescriptions fabricate a false belief that something outside of us will fix us. But the pill doesn't do the healing. The recognition that help is required and the behaviors of seeking out and asking for help are the actions that led to the acquisition of the medication that will play a part in the treatment of whatever ails you. Similarly, when it comes to existential dread, the remedy will come about through concerted action. It is not enough, in other words, to sit in a room with people and agree that we "get" a joke about a cycle of thinking that ultimately defeats us, makes us depressed, produced anxiety, or whatever. "I'm amazing. I hate myself. I'm not real. That's exactly how it goes." Good. We have words to name a feeling and a process, but more steps are required. For starters, we need to intervene in the cycle.
One way to do this, after introducing the meme to a group, is to challenge people to ask each other a question throughout the day, "Where are you in the cycle right now?" I hear the question, I laugh, and I respond: "Ha. I'm amazing right now." "Give it time," you'll say. "Let me know when you don't exist." We laugh together. And at what are we laughing? We are laughing now at three things: 1. It is true that I think in this self-defeating and perplexing way. 2. I know others see me thinking in this way, and I know they can see me because they, too, think in this way. 3. We're working together to do something about it. One laugh moves through many states, from the surprise of recognition to the joy of connection with others to the hope of producing a different mode of being.
Once something typically hidden becomes visible and we verify that, yes, this is the case, and once we unite with others who suffer in similar ways with us, then we can turn to the work of producing healing. One of the many drawbacks of Western medicine's reliance on pharmacology is that the pervasiveness of pills and prescriptions fabricate a false belief that something outside of us will fix us. But the pill doesn't do the healing. The recognition that help is required and the behaviors of seeking out and asking for help are the actions that led to the acquisition of the medication that will play a part in the treatment of whatever ails you. Similarly, when it comes to existential dread, the remedy will come about through concerted action. It is not enough, in other words, to sit in a room with people and agree that we "get" a joke about a cycle of thinking that ultimately defeats us, makes us depressed, produced anxiety, or whatever. "I'm amazing. I hate myself. I'm not real. That's exactly how it goes." Good. We have words to name a feeling and a process, but more steps are required. For starters, we need to intervene in the cycle.
One way to do this, after introducing the meme to a group, is to challenge people to ask each other a question throughout the day, "Where are you in the cycle right now?" I hear the question, I laugh, and I respond: "Ha. I'm amazing right now." "Give it time," you'll say. "Let me know when you don't exist." We laugh together. And at what are we laughing? We are laughing now at three things: 1. It is true that I think in this self-defeating and perplexing way. 2. I know others see me thinking in this way, and I know they can see me because they, too, think in this way. 3. We're working together to do something about it. One laugh moves through many states, from the surprise of recognition to the joy of connection with others to the hope of producing a different mode of being.

Want to carry the work of healing from a group therapy room or a small cohort of friends to the world at large? Don't worry. There's a meme for that.
If I walk through the mechanics of the healing laugh with a group of people in Asheville, NC, and then show them the Tattoo Artist/People Who Need Therapy meme, lots of healing laughter erupts. Working in a substance use treatment center was hands-down the greatest place to produce such laughter because everyone in there, me include, is covered in tattoos. Everyone has some knowledge of the intriguing, medicinal pain that comes through tattooing, and everyone knows that money will sooner go toward the next tattoo than it will toward the deductible on your insurance that enables you to keep going to therapy.
This meme does quite a lot of work. It draws attention to a visible mark that will show itself out on the streets, and once it makes itself visible there it will have the power to continue the healing work started in the therapy room. I'm walking on the sidewalk and I pass in front of a tattoo parlor. I remember, "Ha, I wonder if anyone in there should be getting therapy instead?!" I look at my own tattoos. I need therapy. This is how it is. The work is continuous, and so many people would benefit from doing it. The knowledge produced through this train of thought is almost totally overwhelming. In certain cases, I would be crying as I thought about how many people are suffering, how many institutions perpetuate suffering, how many individuals seek out remedies, often through non-sustainable means. But right now I'm laughing as I face the same kind of overwhelm.
Laughter has the power to heal provided that the laugher rides the wave of the laugh into action for sustaining change in a world that prefers repetition of the same to revolution-like interventions. For something to change, a full-on political revolution is not always needed. The change can start from a tiny laugh in a small room with others who are suffering. As long as you know that that the laugh is awaiting you in the world, that you can and should seek it out, and that, once you find it, you will gain a short-lived boost of energy to intervene, then you are prepared to produce the work of healing in the world.
If I walk through the mechanics of the healing laugh with a group of people in Asheville, NC, and then show them the Tattoo Artist/People Who Need Therapy meme, lots of healing laughter erupts. Working in a substance use treatment center was hands-down the greatest place to produce such laughter because everyone in there, me include, is covered in tattoos. Everyone has some knowledge of the intriguing, medicinal pain that comes through tattooing, and everyone knows that money will sooner go toward the next tattoo than it will toward the deductible on your insurance that enables you to keep going to therapy.
This meme does quite a lot of work. It draws attention to a visible mark that will show itself out on the streets, and once it makes itself visible there it will have the power to continue the healing work started in the therapy room. I'm walking on the sidewalk and I pass in front of a tattoo parlor. I remember, "Ha, I wonder if anyone in there should be getting therapy instead?!" I look at my own tattoos. I need therapy. This is how it is. The work is continuous, and so many people would benefit from doing it. The knowledge produced through this train of thought is almost totally overwhelming. In certain cases, I would be crying as I thought about how many people are suffering, how many institutions perpetuate suffering, how many individuals seek out remedies, often through non-sustainable means. But right now I'm laughing as I face the same kind of overwhelm.
Laughter has the power to heal provided that the laugher rides the wave of the laugh into action for sustaining change in a world that prefers repetition of the same to revolution-like interventions. For something to change, a full-on political revolution is not always needed. The change can start from a tiny laugh in a small room with others who are suffering. As long as you know that that the laugh is awaiting you in the world, that you can and should seek it out, and that, once you find it, you will gain a short-lived boost of energy to intervene, then you are prepared to produce the work of healing in the world.